
In pharmaceutical research and development today, record numbers of molecules are entering clinical development, yet molecule attrition is increasing, especially in Phase II where efficacy is first assessed.
Key opinion leaders within the industry recommend that clinical investigations to find out whether a molecule is efficacious take place as early as possible. Techniques such as incorporating biomarkers and conducting combined Phase Ia/Ib studies can help to address this. However, these changes in study design do not address the underlying productivity limitations in the way industry supports early clinical development.
Pharmaceutical research and development organizations (small to mid-size biotech companies) are structured into functional silos, broadly reflecting the structure of legacy large pharmaceutical companies, with drug substance and drug product teams separate to clinical development teams. This structure is also reflected in outsourcing organizations and has resulted in the formation of separate contract development and manufacturing organizations (CDMOs) and contract research organizations (CROs).
To conduct an early development program, teams need to develop formulations, either manufacture a drug product or establish pharmacy compounding methods, and provide material to a separate clinical site for dosing. Where a manufactured drug product is applied, it must be available in sufficient dose strengths, be manufactured at sufficient scale, and have sufficient stability to complete the clinical trial before the product expires, ideally without resupplies. This adds considerable development time and cost to an early development program.
The implications are even more significant where a candidate molecule may have sub-optimal physicochemical or biopharmaceutic properties. The global pharmaceutical industry today has a pipeline of molecules that are inherently difficult to formulate, with approximately 70–80% of new chemical entities (NCE's) considered poorly soluble and requiring formulation technology to improve the chances of success.
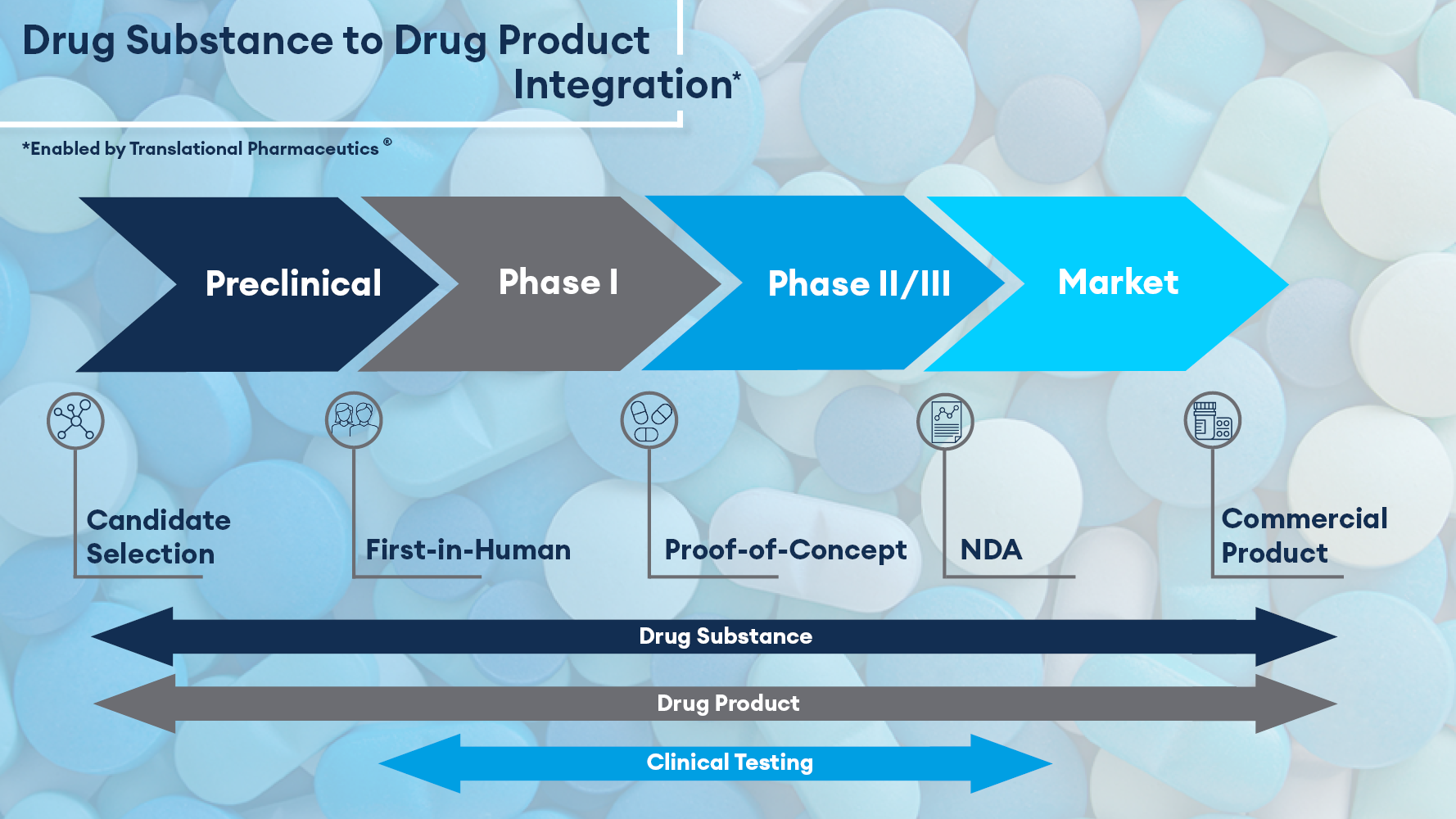
Integrated development strategies for FIH
While innovation can occur under this siloed structure, productivity challenges remain unless an integrated development approach is used. Quotient Sciences can address this with fully integrated drug substance, drug product, and clinical testing services, all within one organization, with our unique Translational Pharmaceutics® platform.
With Translational Pharmaceutics®, drug product is manufactured within days of clinical dosing, minimizing the amount of drug product stability data required (on average 7–14 days) to achieve authorization to run the clinical study. Batch sizes are limited to the amount required to support the immediate clinical need, so the large overages required to support conventional supply chains are removed. This is all achieved under the oversight of a single, multi-disciplinary project manager.
Translational Pharmaceutics® allows the adoption of an adaptive chemistry, manufacturing, and controls (CMC) strategy and an adaptive clinical protocol to maximize the potential for success in Phase I trials. Clinical data from one study period or cohort determines the formulation composition manufactured and dosed in the next.
Within a typical FIH program, where single and multiple ascending doses are administered, the required treatments are achieved using multiples of unit doses manufactured by an external CDMO. In contrast, Translational Pharmaceutics® allows the adaption of the drug product in real-time to deliver a tailored product to meet clinical requirements, minimizing the need to take large quantities of tablets or capsules. This drug product adaption typically comprises a modification in dose during Phase I ascending-dose trials, but it can also be used to switch to an alternative drug product formulation that may be more appropriate for patient administration (for example, changing a suspension to a capsule formulation) or could involve moving to an enabled formulation to respond to emerging drug solubility challenges.
Data from Translational Pharmaceutics® programs analyzed by Joseph DiMasi of the Tufts Center for the Study of Drug Development (CSDD) conclude that this integration alone has the potential to save over 12 months from the development timeline.
FIH case study
JNJ-38877618, a highly selective c-Met tyrosine kinase inhibitor with significant in-vivo anti-tumor activity, was nominated for advancement to FIH trials, which could be conducted in healthy volunteers due to its favorable pre-clinical profile. A key study goal was to commence dosing of a randomized, double-blind, placebo-controlled, FIH trial as quickly as possible, with a formulation that supported immediate progression to ambulatory clinical trials.
A solution formulation with excellent pre-clinical bioavailability was applied to allow for rapid study start-up. However, that solution formulation was not anticipated to be suitable for longer-term ambulatory trials, so two capsule formulations, based upon a spray-dried dispersion of the drug, were incorporated into the trial. The CMC package for the trial included batch analysis and a 7-day stability dataset from demonstration batches of each product, with an option to extend shelf life as further stability data emerged.
Dosing commenced using the solution formulation given the high confidence in achieving human bioavailability, and once initial human safety, tolerability, and pharmacokinetics had been established, a formulation selection was conducted by evaluating the two capsule formulations against the solution formulation in separate cohorts of subjects at the same dose level. This data allowed for the selection of the optimal unit dose formulation to complete single-ascending-dose and multiple-ascending-dose assessments, which continued to be manufactured in real-time under the Translational Pharmaceutics® platform.
The use of a Translational Pharmaceutics® approach enabled Janssen to advance their FIH program from the start of laboratory work to completion of the clinical study in less than 10 months. Efficient, real-time, adaptive GMP (Good Manufacturing Practice) manufacturing of the drug product allowed rapid study start-up by minimizing drug product stability timeframe requirements. A flexible protocol design and adaptive CMC strategies enabled the selection of the drug product to be applied in Phase II, and the assessment of dosing regimens and food effects within a single protocol, avoiding the need for a separate bioavailability study.
Integrated strategies to support POC studies
The strategies described so far have focused on accelerating evaluations in healthy volunteers to demonstrate safety, tolerability, and human drug exposures using Translational Pharmaceutics®. However, further benefits can be achieved by maintaining integration when transitioning to POC studies, using manufacturing experience established during the healthy volunteer phase to supply drug product to patient sites.
In one such example, a sponsor was developing a new chemical entity (NCE) for an orphan disease and applied Translational Pharmaceutics® to deliver the FIH trial. As a rare disease, however, patient recruitment rates were unpredictable and required the establishment of multiple potential clinical centres globally. Quotient Sciences continued to support drug product manufacture in real-time as patients were recruited, ensuring seamless drug product supply without the need to transfer the manufacturing process to another partner.
Conclusions
The pharmaceutical industry is constrained by a legacy structure that extends the time to transition a new molecule from candidate selection to FIH, and through early clinical studies to POC. An integrated service provider can shorten timelines to POC by over 12 months by:
- identifying the right formulation approach for the drug
- supporting early development studies using Translational Pharmaceutics® to:
- minimize the amount of drug product stability data required to get the study running
- focus manufacturing activity on drug product needed to dose
- remove the need for large-scale drug product manufacturing
- support transition to patient-appropriate formulations
- providing a seamless transition to supply of drug product for global POC studies.
For more information about Quotient Sciences’ fully integrated Translational Pharmaceutics® platform, click here.